Table of Content


Key Takeaways
- Pharmacy management software development means building systems that handle prescriptions, inventory, billing, patient records, compliance, and integrations for pharmacy operations.
- US-ready builds need HIPAA, DEA EPCS, DSCSA, HL7/FHIR, and NCPDP compliance designed in from day one, not added before launch.
- Compliance-first architecture beats a generic features-and-cost approach because EPCS identity, DSCSA tracing, and HIPAA audit logs touch the same data tables your features do.
- Cost depends on the pharmacy model. An MVP, a multi-store retail platform, and a hospital-grade system carry different price tags and different risk profiles.
Table of Content
Every pharmacy leader evaluating vendors eventually asks the same question: Does this system know what happens when something breaks? Not the demo, the real failure modes.
The 2 am EPCS credential failure. The DSCSA verification call times out. The EHR update that silently drops a prescription change. That question, more than any feature checklist, decides which vendor gets the contract.
Not sure if your current system covers DEA EPCS and DSCSA?
What Is Pharmacy Management Software Development?
Pharmacy management software development is the process of building systems that run a pharmacy’s core operations: prescription processing, inventory control, billing, patient records, regulatory compliance, and reporting, in one connected platform.
A pharmacy management system (PMS) typically includes electronic prescribing (eRx), electronic prescribing of controlled substances (EPCS), a dispensing workflow engine, inventory tracking, point-of-sale billing, patient profiles, and analytics.
Each piece has to share data with the others without creating compliance gaps.
Watch Our Video:
Why Are US Pharmacies Investing in Digital Pharmacy Software in 2026?
Pharmacy access in the US has been shrinking for over a decade.
More than 29% of the nearly 89,000 retail pharmacies operating between 2010 and 2020 had closed by 2021, according to a Health Affairs study using National Council for Prescription Drug Programs data
That trend has not slowed. CVS closed roughly 270 stores in 2025 after shutting more than 800 over the prior three years, and Walgreens has been working through about 1,200 additional closures, according to reporting compiled by Lockton.
Fewer physical locations mean each remaining pharmacy needs to do more with less. That is the practical case for investing in digital pharmacy software:
- Multi-location visibility. Chains and healthcare systems need real-time inventory and prescription data across every site, not end-of-day batch syncs.
- Medication safety. Automated interaction checks and dosage verification catch errors before they reach a patient.
- Telepharmacy support. Remote-site dispensing, telemedicine support, and virtual consults keep underserved areas connected to a licensed pharmacist.
- Margin protection. Automated claims and denial management reduce the reimbursement leakage that is driving many closures in the first place.

What Features Should Pharmacy Management Software Include?
A pharmacy management system earns its name by covering the full operational loop, not just dispensing. These are the modules worth building or buying in 2026.
- Prescription services:
eRx intake, EPCS-compliant controlled substance handling, refill authorization, and prior authorization routing.
- Inventory management:
Real-time stock levels, expiration, and recall tracking, multi-wholesaler purchase order automation.
- Sales and POS:
Barcode-driven checkout, insurance adjudication at the register, and split-tender payment support.
- Patient management:
Unified patient profiles, allergy and interaction history, consent, and communication preferences.
- Billing and claims:
Real-time insurance adjudication, claim denial tracking, and patient-responsibility calculation.
- Reporting:
Operational dashboards for fill rates, inventory turns, and compliance audit trails.
- User roles:
Role-based access separates pharmacists, technicians, and front-desk staff by permission level.
- Refill reminders:
Automated SMS, app, and IVR reminders tied to adherence tracking.
- Delivery:
Route optimization and proof-of-delivery for the last-mile medicine delivery and prescription fulfillment.
- Telepharmacy:
Remote verification workflows for licensed pharmacist oversight at unstaffed sites.
- Clinical decision support:
Drug interaction alerts, dosage range checks, and formulary guidance at the point of prescribing.

What HIPAA, DEA EPCS, and DSCSA Rules Affect Pharmacy Software Development?
Three federal frameworks shape almost every architecture decision in pharmacy software. Missing one late in a build is expensive. Missing one after launch is a compliance incident.
| Regulation | Applies To | Product Requirement | Audit Evidence |
| HIPAA Security Rule | Any system storing or transmitting electronic protected health information (ePHI) | Administrative, physical, and technical safeguards protecting ePHI confidentiality and integrity | Documented risk analysis, access logs, encryption records (HHS.gov) |
| DEA EPCS | Software handling Schedule II–V controlled substance prescriptions | Identity-proofed prescriber credentials, two-factor authentication, tamper-evident digital signatures | Daily internal audit review, signed prescription logs, and credential issuance records |
| DSCSA | Manufacturers, wholesalers, and dispensers (pharmacies) | Package-level product tracing and verification, illegitimate product reporting within 24 hours | Transaction information, transaction history, and transaction statement records retained 6+ years (FDA.gov) |
| State pharmacy boards | Licensed pharmacies and telepharmacy sites | State-specific dispensing, delivery, and remote-supervision rules | Varies by state; typically, inspection and licensure records |
HHS proposed a significant strengthening of the Security Rule in December 2024, shifting several currently optional safeguards, like encryption at rest and in transit, to mandatory requirements (Federal Register).
It had not been finalized as of this writing. Building to the stricter standard now avoids a costly retrofit later.
One detail most vendor content skips: DSCSA’s enhanced package-level tracing requirements are already enforced for manufacturers, wholesalers, and large dispensers.
Small dispensers, defined as 25 or fewer pharmacists and technicians, remain exempt until November 27, 2026. If you are building for independent pharmacies, that exemption date changes your compliance timeline.
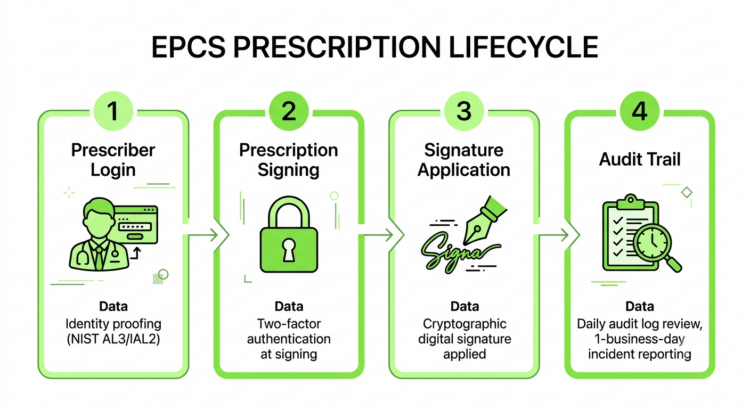
How Do DEA EPCS Requirements Change the Software Architecture?
EPCS is not a feature you bolt onto an existing prescribing module. It changes the identity, authentication, and audit layers underneath everything else.
Three architectural pillars, each mapped to a federal standard, define EPCS compliance:
- Identity proofing:
Prescribers must be verified to Assurance Level 3 of NIST SP 800-63-1, equivalent to Identity Assurance Level 2 under the newer NIST 800-63-3 framework, before they can receive an EPCS credential.
- Two-factor authentication:
Every controlled substance prescription requires two-factor sign-off at the moment of signing, under 21 CFR 1311.115, not just at login.
- Digital signing and audit logging:
Each prescription gets a cryptographic signature tied to the verified prescriber, and the system must run daily internal audits of prescription activity with incident reporting within one business day of a detected anomaly.
Get the identity layer wrong, and every feature built on top of it, including refill automation, PBM integration, and patient messaging, inherits the same compliance gap.
How Do HL7, FHIR, NCPDP, EHR, PBM, and eRx Integrations Work?
A pharmacy system that cannot talk to the outside world is a very expensive spreadsheet. Interoperability runs through two standards families.
HL7’s FHIR (Fast Healthcare Interoperability Resources) defines the data structures that let a pharmacy system exchange medication data with EHRs.
The MedicationRequest resource represents a medication order from a prescriber. The MedicationDispense resource represents the pharmacy’s fulfillment of that order (HL7.org).
NCPDP SCRIPT is the messaging standard most US eRx networks run on, connecting prescribers, pharmacies, and PBMs for new prescriptions, refill requests, and cancellations.
Together, FHIR and NCPDP SCRIPT let a pharmacy system plug into Surescripts, major EHR platforms, and PBM adjudication networks without custom point-to-point integrations for every partner.
What Tech Stack Is Best for Pharmacy Management Software Development?
There is no single correct stack, but there is a consistent pattern among systems built for HIPAA-regulated, high-availability pharmacy workloads.
| Layer | Recommended Technology |
| Frontend and mobile | React or Next.js for web, React Native or Flutter for pharmacist and patient apps |
| Backend | Java with Spring Boot, or Node.js and .NET, depending on team expertise and existing enterprise stack |
| Database | PostgreSQL for transactional data, Redis for caching, Kafka for event streaming between services |
| Interoperability | FHIR APIs, NCPDP SCRIPT connectors |
| Cloud and security | AWS or Azure HIPAA-eligible services, with encryption at rest and in transit |
| Analytics and DevOps | Dedicated analytics pipeline separate from transactional database, CI/CD with compliance-gated deployment checks |
Code Brew Labs structures EPCS compliance directly into the data layer.
How Much Does It Cost to Develop Pharmacy Management Software in the USA?
Cost depends far more on integration count and compliance depth than on screen count. A system with five or more required integrations, PBM, EHR, state prescription monitoring, wholesaler feeds, should budget well above baseline estimates.
| Tier | Investment Range | Best Fit |
| MVP | $80,000–$180,000 | Independent pharmacies, early-stage startups validating core workflows |
| Advanced retail or multi-store | $180,000–$500,000 | Regional chains needing multi-location sync and deeper integrations |
| Hospital or enterprise platform | $500,000–$1,000,000+ | Health systems and PBMs with EHR-grade interoperability and validation needs |
These ranges hold up against current market data. One 2026 industry analysis found custom pharmacy software costing $30,000 to $250,000, depending on integration depth (Citrusbug), which sits comfortably within the MVP-to-advanced range above.
Total cost of ownership matters more than build cost alone. A system that costs $200,000 to build but requires $60,000 a year in maintenance and compliance updates carries a five-year TCO of $500,000, not $200,000 (Pharmacy Business).
Budget for maintenance from the first proposal, not after the first invoice.
Primary cost drivers, in rough order of impact: integration count and complexity, EPCS and identity infrastructure, data migration from legacy systems, cloud and security architecture, ongoing compliance audits, and AI or automation features layered on top.
How Do You Build Pharmacy Management Software Step by Step?
A compliance-first build follows a specific sequence. Skipping ahead to development before the compliance blueprint is set is the single most common cause of expensive rework.
Discovery:
Map current workflows, pain points, and required integrations.
Workflow mapping:
Document dispensing, billing, and patient-management flows in detail.
Compliance blueprint:
Define HIPAA, EPCS, and DSCSA requirements before any UX work starts.
UX and architecture:
Design interfaces and system architecture around the compliance blueprint, not around it.
MVP build:
Ship core prescribing, inventory, and billing first.
Integrations:
Connect EHR, PBM, and state PDMP systems.
Security testing:
Penetration testing and HIPAA risk assessment before the pilot.
Pilot:
Run in one location with close monitoring before wider rollout.
Data migration:
Move legacy records with validation checks at every step.
Training and launch:
Train staff, then launch with a rollback plan ready.
Post-launch support:
Monitor, patch, and maintain compliance documentation continuously.
Should You Build Custom, Buy SaaS, or Use White-Label Pharmacy Software?
The right path depends on how specific your workflows are, not on budget alone.
| Pharmacy Type | Recommended Path |
| Startups and new independents | SaaS or white-label for fast, compliant launch |
| Independent pharmacies | SaaS, with custom modules only for a specific niche, like compounding |
| Regional chains | Custom or heavily configured platform for multi-location sync |
| Hospital systems | Custom-built, given deep EHR and closed-loop medication requirements |
| Specialty pharmacies | Custom, because 340B, compounding, or LTC workflows rarely fit off-the-shelf tools |
| Enterprise and PBM networks | Custom, built for scale, validation, and proprietary competitive advantage |
What AI, Automation, and Future Trends Matter in Pharmacy Management Software for 2026?
AI in pharmacy software works best where it removes repetitive judgment calls, not clinical ones. The technologies gaining real traction in 2026:
- Demand forecasting and smart replenishment:
Predictive ordering that reduces both stockouts and expired inventory write-offs.
- Anomaly detection:
Flagging unusual dispensing patterns for controlled substances before they become a diversion problem.
- Claim denial prediction:
Catching likely claim rejections before submission, not after the remittance comes back.
- Patient adherence nudges:
Personalized refill timing based on actual fill history, not a fixed 30-day reminder.
- Prescription direction simplification:
Converting clinical dosing language into plain-language instructions patients actually follow.
- Human-in-the-loop safety:
Every AI-flagged interaction or anomaly routes to a pharmacist for final judgment. No fully autonomous clinical decisions.
The pharmacy automation market is projected to keep growing steadily through 2030 (Verified Market Research), which means AI features built today need architecture flexible enough to absorb next year’s model, not just this year’s.
What Implementation Challenges Delay Pharmacy Software Projects?
The features rarely cause delays. These operational realities do:
- Legacy data quality:
Years of inconsistent records make migration slower than any vendor estimates upfront.
- EHR integration friction:
Hospital EHR vendors move slowly, and integration timelines are rarely in your control.
- Staff adoption:
A technically perfect system that pharmacists route around at the counter has failed.
- Controlled substance workflow complexity:
EPCS touches identity, hardware, and process simultaneously.
- State-by-state variation:
Multi-state operators face different telepharmacy and delivery rules in every jurisdiction.
- Security review cycles:
Enterprise security reviews for HIPAA-regulated systems routinely add 4–8 weeks.
- Payer connectivity gaps:
PBM onboarding timelines are often the longest single dependency in the project plan.
How Code Brew Labs Can Help Develop Pharmacy Management Software
Most vendors sequence a build around features first and compliance later. That sequencing is backward, and it is why so many pharmacy software projects blow their budget on rework. Our framework runs in a fixed order:
Compliance:
HIPAA, EPCS, and DSCSA requirements shape the data model before a single screen is designed.
Workflows:
Real pharmacist and technician workflows, not idealized ones, drive the UX.
Integrations:
EHR, PBM, and PDMP connections get built once the compliance and workflow foundation is stable.
Automation:
AI and automation layer onto a system that already works, not instead of one that does.
Scale:
Multi-location and enterprise scaling come last, because scaling a non-compliant system just multiplies the risk.
Pharmacy management software is not a features-and-cost decision anymore. It is infrastructure that determines whether a pharmacy can dispense safely, stay compliant across three federal frameworks, and stay visible across every location it operates.
The pharmacies and health systems that treat compliance as the starting architecture, not a phase added before launch, are the ones that scale without expensive rework. Everything else, the AI features, the automation, the multi-location dashboards, works only if that foundation holds.
FAQs
How much does it cost to develop pharmacy management software?
Costs typically range from $80,000 for a focused MVP to over $1,000,000 for a hospital-grade enterprise platform. Integration count, EPCS infrastructure, and compliance depth drive most of the variation between projects.
How long does pharmacy management software development take?
An MVP typically takes 3 to 5 months. Advanced multi-store platforms run 76 to 10 months, and hospital or enterprise systems with deep EHR integration commonly take 12 to 18 months.
What HIPAA requirements apply to pharmacy software?
Any system storing or transmitting electronic protected health information needs administrative, physical, and technical safeguards under the HIPAA Security Rule, backed by a documented risk analysis and access controls.
What is DEA EPCS, and why does it matter for pharmacy software?
EPCS is the DEA framework governing electronic prescribing of controlled substances. It requires identity-proofed prescriber credentials, two-factor authentication at signing, and daily audit logging, and it shapes core system architecture, not just one feature.
What are the must-have features in pharmacy management software?
Prescription services, inventory management, billing and claims, patient management, reporting, and clinical decision support form the core. Telepharmacy and delivery matter for pharmacies serving distributed or rural populations.
What is the best tech stack for pharmacy management software development?
A common, proven pattern uses React or Next.js frontends, Java Spring Boot or Node.js backends, PostgreSQL and Redis for data, and FHIR APIs for interoperability, deployed on HIPAA-eligible AWS or Azure infrastructure.
What integrations does pharmacy software need?
EHR systems via HL7 FHIR, PBM networks for claims adjudication, state prescription drug monitoring programs, and eRx networks like Surescripts using the NCPDP SCRIPT standard.
Should I choose custom software or a SaaS platform?
SaaS or white-label solutions fit startups and independents needing fast, compliant launches. Custom builds fit hospital systems, specialty pharmacies, and enterprises whose workflows do not fit standardized software.
Let's Convert Your Business Idea Into Success!
Free Consultation from Top Industry Experts
Let’s Build Your Dream App!
Share article on :





Ready To Fuel Your Vision With AI-Powered Innovation?





Level- 18, Dubai World Trade Centre Tower, Sheikh Rashid Tower, Sheikh Zayed Rd, Dubai, UAE
business@code-brew.com +971-55-645-7972
Plot no I - 36, Sector 83 Alpha, Mohali SAS Nagar 140308
business@code-brew.com +91-771-976-8427
Av. Miguel Hidalgo y Costilla 1995, Arcos Vallarta, 44600 Guadalajara, Mexico
business@code-brew.com +1(213)2614953
4231 Balboa Ave #512 San Diego, CA 92117 United States
business@code-brew.com +1(213)2614953
2nd floor, College House, 17 King Edwards Rd, London HA4 7AE, UK
business@code-brew.com +44 (20) 82644493
Partner With Experts Who Leverage AI & Tech To Transform Ideas Into Market-Leading Solutions.
Wait! Looking for Right Technology Partner For Your Business Growth?
It's Time To Convert Your Business Idea Into Success!
Get Free Consultation From Top Industry Experts:
I would like to keep it to myself